Patient Information
& Services
Chiropractic Care Services
-
Spinal Manipulation
-
Activator
-
SOT (Sacro-Occipital Technique)
-
Drop Techniques
-
Cervical Traction/Distraction
-
Chiropractic Biophysics
-
Exercise Prescription
-
Nutrition
-
Custom Orthotics
-
Cox Flexion Distraction (F & D)
Soft Tissue Therapy Services
-
Soft Tissue Therapy
-
Sports Massage Therapy
-
Accident Therapy
-
Nimmo Receptor Tonus Tech.
-
Manual Active Release.
Acupuncture Services
-
Needle Acupuncture
-
Medical Acupuncture
-
Neurofunctional Acupuncture
-
Bio-Electric Acupuncture
-
Auricular Acupuncture
-
Acupressure
-
Cupping
-
Gua Sha
-
Stress Management Acupuncture
Nutrition Services
-
General Health Nutrition
-
Accident Rehabilitation
-
Nutrition
-
Sports
-
Supplementation Nutrition
-
Nutrition for Weight Loss
Physiotherapy Services
-
Electrical Stimulation
-
Interferential
-
EMS
-
TENs
-
Russian
-
Ultrasound
-
Cryotherapy/Thermotherapy
-
Neuro-Kinetic Exercises
-
Personal Training
Custom Orthotics Services
-
Custom Orthotic Inserts
-
State of the Art 3D CAD Scanning
-
Gait Analysis
-
Postural Analysis
-
Biomechanical Analysis
-
EA Foam Orthotics
Understanding Spinal Biomechanics & Pain


Proper Posture is essential for overall health. Without proper posture, our body is in a constant state of stress which leads to bone, muscle, joint and nervous system stress.
Better posture = less pain and better long-term health. See below.
Spinal Biomechanics
Proper Spinal posture is critical because it directly governs how efficiently the vascular system, muscular system, cerebral spinal fluid and nervous system perform. The spine is not just a structural support; it’s your bodies fuse box.
When posture is optimal, joints move properly, muscles balance appropriately, and neural/vascular/CSF input/output remains clear and coordinated.
However, poor posture (such as forward head carriage or pelvic imbalance), loss of spinal stability or severe degeneration creates abnormal joint stress and sustained muscle tension, alterations in proprioceptive, CSF flow and blood flow to the brain.
Over time, the brain adapts to these distorted signals as a new “normal,” reinforcing dysfunctional movement patterns with protective muscle guarding, which is called muscle splinting.
This can lead to a cascade of effects, including chronic pain, reduced mobility, impaired coordination, hormonal changes and even changes in autonomic function such as headaches, fatigue, and brain fog.
Blow we will discuss how spinal postural changes affect:
-
Spinal Discs
-
Spinal Facet Joints
-
Spinal Ligaments
-
Nervous System
-
Cerebral Spinal Fluid Flow
-
HPA Axis - Stress Response
-
Brain Function
-
Pain Perception


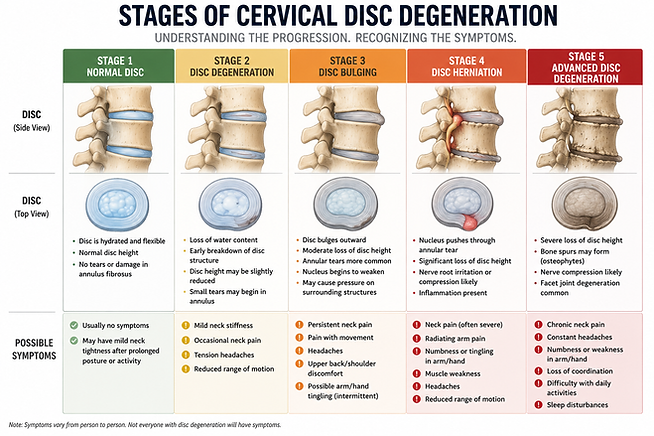
Disc Degeneration
The primary function of the intervertebral disc is to absorb and transmit axial compressive loading through the spinal column and to control loading by distributing stresses within the dense fibrocartilage of its annulus fibrosus. Abnormal cervical spine posture, including loss of normal lordosis or forward head positioning, alters load distribution across the disc, resulting in increased anterior or posterior stress concentrations. This leads to abnormal strain within the annular fibers, accelerated disc degeneration, reduced disc height, and increased risk of annular fissuring and herniation. Over time, these biomechanical alterations compromise the disc’s ability to effectively dissipate forces, contributing to chronic spinal dysfunction, degeneration and pain.
-
Yoganandan, Narayan; Nahum, Alan M.; Melvin, John W.; The Medical College of Wisconsin Inc. Accidental Injury: Biomechanics and Prevention (p. 551). Springer New York. Kindle Edition.

Facet Joint Degeneration
Facet joints are paired synovial joints located at the back of each spinal segment. Their main functions are:
-
Guide and control spinal motion
-
Prevent excessive rotation, flexion, and extension
-
-
Stabilize the spine
-
Work with discs to maintain spinal segment integrity
-
-
Distribute load
-
Share weight-bearing forces with intervertebral discs
-
-
Limit shear forces
-
Prevent vertebrae from sliding abnormally
-
-
Protect the disc
-
Reduce excessive stress on the intervertebral disc during movement
-
Facet joint osteoarthritis (FJ OA) is a degenerative condition affecting the facet (zygapophyseal) joints of the spine. It is strongly associated with degenerative disc disease and is now understood as part of a whole spinal motion-segment failure.
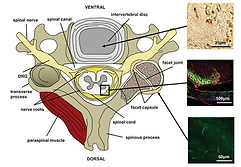
Cervical facet joints have been well established in the literature as a common source of axial neck pain, with an estimated prevalence up to 66%. The diarthrodial joints are formed by bony articulation of the SAP and inferior articular process, surrounded by a fibrous capsule; they contain articular cartilage and menisci and are innervated by the medial branches of the dorsal rami. Pain from the cervical facet joints can originate from traumatic hyperextension injuries such as whiplash or degenerative processes such as osteoarthritis.

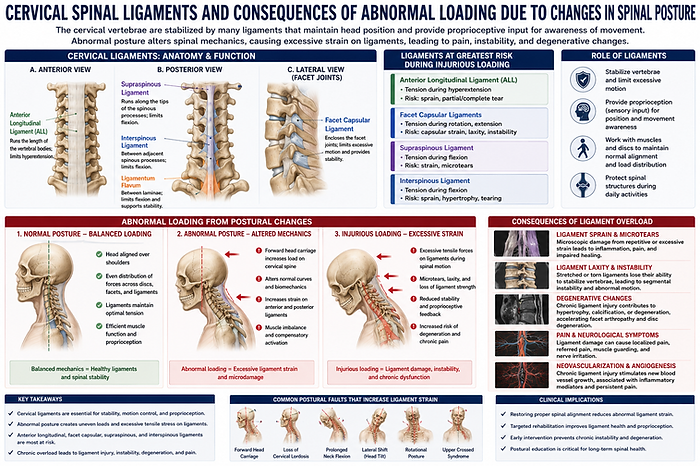
Spinal Ligament Injury
The cervical vertebrae are stabilized by many ligaments in both the anterior and posterior regions of the spine that normally contribute to maintaining the head position and providing neck proprioception, which is the sensory input that aids in awareness of relative position and movement of the body during spinal motions. The ligaments in the cervical spine include the anterior and posterior longitudinal ligaments that span the entire vertebral column, ligaments that connect pairs of adjacent vertebrae (ligamentum flavum, interspinous, and supraspinous ligaments), and the bilateral facet capsular ligaments that enclose the apposing surfaces of the articular pillars of adjacent vertebrae. The anterior longitudinal, facet capsular, supraspinous, and interspinous ligaments are at particular risk for undergoing excessive strain during injurious loading of the cervical spine, because of their role in bearing tensile loads during spinal motion.
In addition to proprioception and structural support, numerous immunohistochemical studies have reported the longitudinal, supraspinous, interspinous, and facet capsular ligaments to be innervated by nociceptive fibers (pain fibers) and free nerve endings. Histological studies have also identified low and high threshold mechanoreceptors, based on visualization of specialized sensory terminals, in many of these same spinal ligaments, along with nociceptive innervation. The capacity of nerve fibers in spinal ligaments to be activated by a wide range of mechanical loading modalities further suggests their role in initiating and/or signaling painful loading from cervical spine injuries due to excessive loading of those tissues.
-
Yoganandan, Narayan; Nahum, Alan M.; Melvin, John W.; The Medical College of Wisconsin Inc. Accidental Injury: Biomechanics and Prevention (p. 552). Springer New York. Kindle Edition.




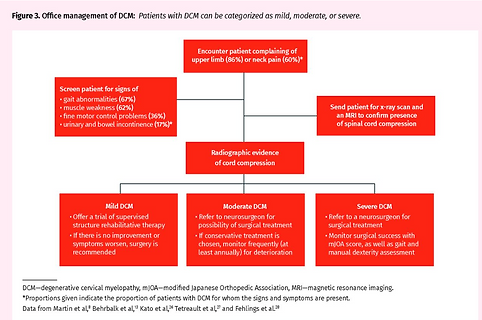
Myelopathy
Degenerative cervical myelopathy comprises age-related degenerative pathologies of the cervical spinal column that lead to myelopathy from compression of the spinal cord. These include osteoarthritic degeneration (cervical spondylosis) and ligamentous aberrations (ossification of the posterior longitudinal ligament or ligamentum flavum
-
Witiw CD, Fehlings MG: Degenerative cervical myelopathy. CMAJ | JANUARY 23, 2017 | VOLUME 189 | ISSUE 3




Fatty Infiltration
Loss of normal spinal movement is associated with progressive neuromuscular degeneration and structural deterioration of the spinal stabilizing tissues. When spinal segments become hypomobile due to pain, ligament injury, disc pathology, joint dysfunction, or protective muscle guarding, the deep stabilizing musculature, particularly the multifidus and other paraspinal muscles undergo reflex inhibition and reduced activation.
Over time, this disuse and altered neuromuscular control contribute to muscle atrophy, reduced oxidative capacity, and fatty infiltration within the spinal musculature. These changes impair spinal stability, proprioception, and load distribution, creating a cycle of chronic dysfunction, persistent pain, and further degeneration.
Studies have demonstrated that reduced spinal movement and chronic low back or cervical pain are associated with increased fatty infiltration of the multifidus muscles, decreased cross-sectional muscle area, and progressive degenerative changes involving the discs, facet joints, and supporting connective tissues.
Restoration of spinal mobility and neuromuscular activation is therefore considered an important component in reducing ongoing degeneration and improving spinal function.



Cerebral Spinal Fluid and Blood Flow changes
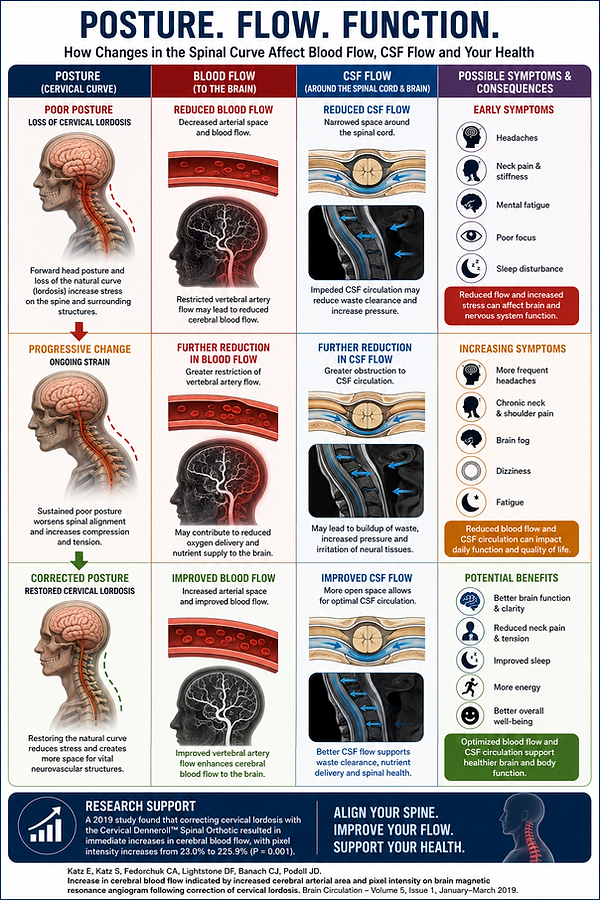
Research suggests that the natural curve of the neck plays an important role in neurological and vascular function. The cervical spine surrounds and protects critical structures involved in cerebral blood flow and cerebrospinal fluid (CSF) circulation. When the cervical lordosis becomes reduced or abnormal, altered biomechanics, muscular tension, and ligament stress may contribute to changes in spinal motion, vascular dynamics, and neural function. Restoration of normal cervical alignment may help improve the mechanical environment surrounding the spinal cord, vertebral arteries, and CSF pathways.
In a 2019 study published in Brain Circulation, researchers evaluated brain magnetic resonance angiograms (MRA) before and after cervical lordosis correction using the Cervical Denneroll Spinal Orthotic. The investigators found statistically significant increases in cerebral blood flow following cervical curve correction, with measured increases in arterial pixel intensity ranging from 23.0% to 225.9% (P = 0.001). These findings suggest that improving cervical spinal alignment may positively influence blood flow to the brain and potentially support healthier neurological function.
Because cerebrospinal fluid circulation and cerebral blood flow are closely linked to posture, spinal motion, and upper cervical mechanics, maintaining proper spinal alignment may be an important component of optimizing neurological health, reducing mechanical stress on the nervous system, and supporting overall brain and spinal cord function.
Pain and Spinal Posture
Pain. This most commonly results from trauma and/or injury, with the spine as the most common injury site for producing chronic pain. When considering the topic of pain, it is important to define that pain is a combination of sensory and emotional experiences and nociception is the set of physiological responses that transmit the pain signals. Hyperalgesia and allodynia are two primary classes of behavioral responses. Hyperalgesia is an amplified response to a stimulus (mechanical, temperature or chemical) and suggests that more pain is perceived. Allodynia is characterized as pain that is evoked by a typically non-noxious stimulus. Hyperalgesia and allodynia provide quantitative measures of pain that relate to the clinical presentation of symptoms and why your spinal biomechanics can predict your pain outcome.
-
Yoganandan, Narayan; Nahum, Alan M.; Melvin, John W.; The Medical College of Wisconsin Inc. Accidental Injury: Biomechanics and Prevention (p. 549). Springer New York. Kindle Edition.

Pain Cycle by Dr. Ming Kao of Stanford Medicine Pain Lab
Altered Biomechanics (Blue Arrow) results after the pain experience, and contributes to:
Pain
Altered Biomechanics
Myofascial Pain
Reflexive Guarding
Overuse Injury
Nerve Entrapment
Metabolic Dysfunction
Immune System Dysfunction
Hormone Dysfunction
Changes in Spinal Posture Trigger Mechanical Pain Signals to the Brain

Changes in Spinal Posture Trigger Myofascial (Muscle) Pain Cycle
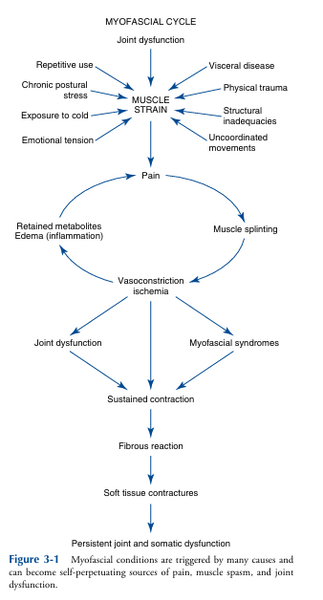
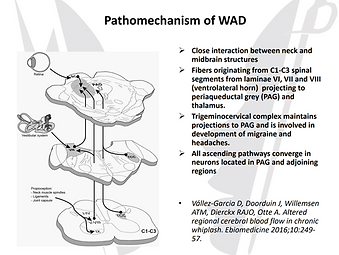
Changes in Spinal Posture Trigger Cervical Nerves 1-3, Trigeminal Nerve, Vagus Nerve and Mid-Brain
Spinal Postural Changes lead to
Altered Spinal Mechanics
Changes in Nervous System Function
Changes in ANS Function
Changes in Blood Flow
Changes in CSF Flow
Spinal Degeneration
Nerve Compression/Injury
S1 Cortex (Brain) Changs
PAIN and LOSS of FUNCTION
Consequence of Chronic Pain
Loss of Gray Matter (Brain Shrinks)
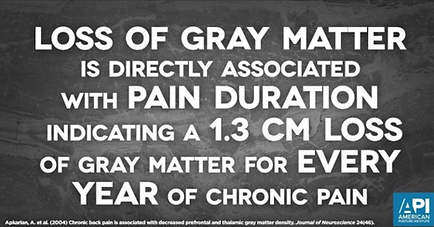

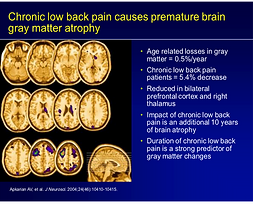
Consequence of Chronic Pain
Appearance of Psychological Issues that are actually a Pain Response